

25 Jun The Definitive Guide to Cholesterol
 Contrary to what we’ve been told, cholesterol didn’t evolve to give us heart disease. It’s not here to kill us. The actual roles of cholesterol in the body include insulating neurons, building and maintaining cellular membranes, participating in the immune response, metabolizing fat soluble vitamins, synthesizing vitamin D, producing bile, and kick-starting the body’s synthesis of many hormones, including the sex hormones. Without cholesterol, it’s true that we wouldn’t have heart disease, but we also wouldn’t be alive.
Contrary to what we’ve been told, cholesterol didn’t evolve to give us heart disease. It’s not here to kill us. The actual roles of cholesterol in the body include insulating neurons, building and maintaining cellular membranes, participating in the immune response, metabolizing fat soluble vitamins, synthesizing vitamin D, producing bile, and kick-starting the body’s synthesis of many hormones, including the sex hormones. Without cholesterol, it’s true that we wouldn’t have heart disease, but we also wouldn’t be alive.
Given all the work cholesterol has to do, the liver is careful to ensure the body always has enough, producing some 1000-1400 milligrams of it each day. Dietary cholesterol is a relative drop in the bucket. And besides, the liver has sensitive feedback mechanisms that regulate cholesterol production in response to how much you get from your diet. Eat more cholesterol, make less in the liver. Eat less, make more in liver.
Now, if cholesterol is so important, why do we worry about it at all? How has it garnered such a bad reputation for giving us heart attacks?
History of Cholesterol and Heart Disease
Heart disease took off in the early part of the twentieth century, and doctors frantically searched for the cause throughout the next several decades. Early studies in rabbits found that feeding them dietary cholesterol reliably increased blood cholesterol levels and induced atherosclerosis that very much resembled human atherosclerosis. Human tests in the fifties initially showed an association between early death by heart disease and fat deposits and lesions along artery walls. Because cholesterol was found to be present in those deposits and because researchers had previously associated familial hypercholesterolemia (hereditary high blood cholesterol) with heart disease, they concluded that cholesterol must be the culprit.
And while it’s true that cholesterol is involved in heart disease, the direct cause-and-effect relationship has not been established. The reality is far more complicated. To get closer to the reality, we must first understand what these cholesterol numbers actually mean.
Cholesterol versus Lipoproteins
Back in those early rabbit studies, researchers discovered a curious thing: even though feeding the rabbits cholesterol spiked their blood cholesterol and gave them heart disease, bypassing the first step and injecting it directly into the blood had no effect. It was completely harmless.
As it turns out, cholesterol doesn’t normally float around the blood by itself. It is contained within lipoproteins. You can think of lipoproteins as delivery vessels. They contain cholesterol, antioxidants, and fatty acids and along the surface have various proteins that direct the lipoprotein to different sites around the body. It’s not the cholesterol that is involved with atherosclerosis. It’s the lipoprotein.
Let’s play the freeway analogy game. Both LDL-cholesterol (LDL-C) and HDL-cholesterol (HDL-C), the standard, basic readings you get from the lab, do not reflect the number of LDL or HDL lipoproteins, or particles, in your serum. Instead, they reflect the total amount of cholesterol contained in your LDL and HDL particles. Hence, the “C” in LDL/HDL-C, which stands for “cholesterol.” Measuring the LDL/HDL-C and then making potentially life-changing health decisions based on the number is like counting the number of people riding in vehicles on a freeway to determine the severity of traffic. It’s data, and it might give you a rough approximation of the situation, but it’s not as useful as actually counting the number of vehicles. A reading of 100 could mean you’re dealing with a hundred compact cars, each carrying a single driver, or it could mean you’ve got four buses carrying 25 passengers each. Or it could be a couple buses and the rest cars. You simply don’t know how bad (or good) traffic is until you get a direct measurement of LDL and HDL particle number.
How does this relate to heart disease?
In my opinion, the most convincing heart disease hypothesis goes like this:
- LDL receptors normally “receive” LDL particles and remove them from circulation so that they can deliver nutrients and cholesterol to cells, and fulfill their normal roles in the body.
- If LDL receptor activity is downregulated, LDL particles clear more slowly from and spend more time in the blood. Particles accumulate.
- When LDL particles hang out in the blood for longer stretches of time, their fragile polyunsaturated fatty membranes are exposed to more oxidative forces, like inflammation, and their limited store of protective antioxidants can deplete.
- When this happens, the LDL particles oxidize.
- Once oxidized, LDL particles are taken up by the endothelium – a layer of cells that lines the inside of blood vessels – to form atherosclerotic plaque so they don’t damage the blood vessel. This sounds bad (and is), but it’s preferable to acutely damaging the blood vessels right away.
- So it’s the oxidized LDL that gets taken up into the endothelium and precipitates the formation of atherosclerotic plaque, rather than regular LDL. OxLDL, poor receptor activity, and inflammation are the problems.
If that’s the case, what exactly is the deal with traditional blood lipid numbers—the ones you get on a standard blood test?
This information is how I view cholesterol as it relates to my individual biology. If you have questions about your cholesterol numbers, discuss them with a qualified health professional.
Total Cholesterol
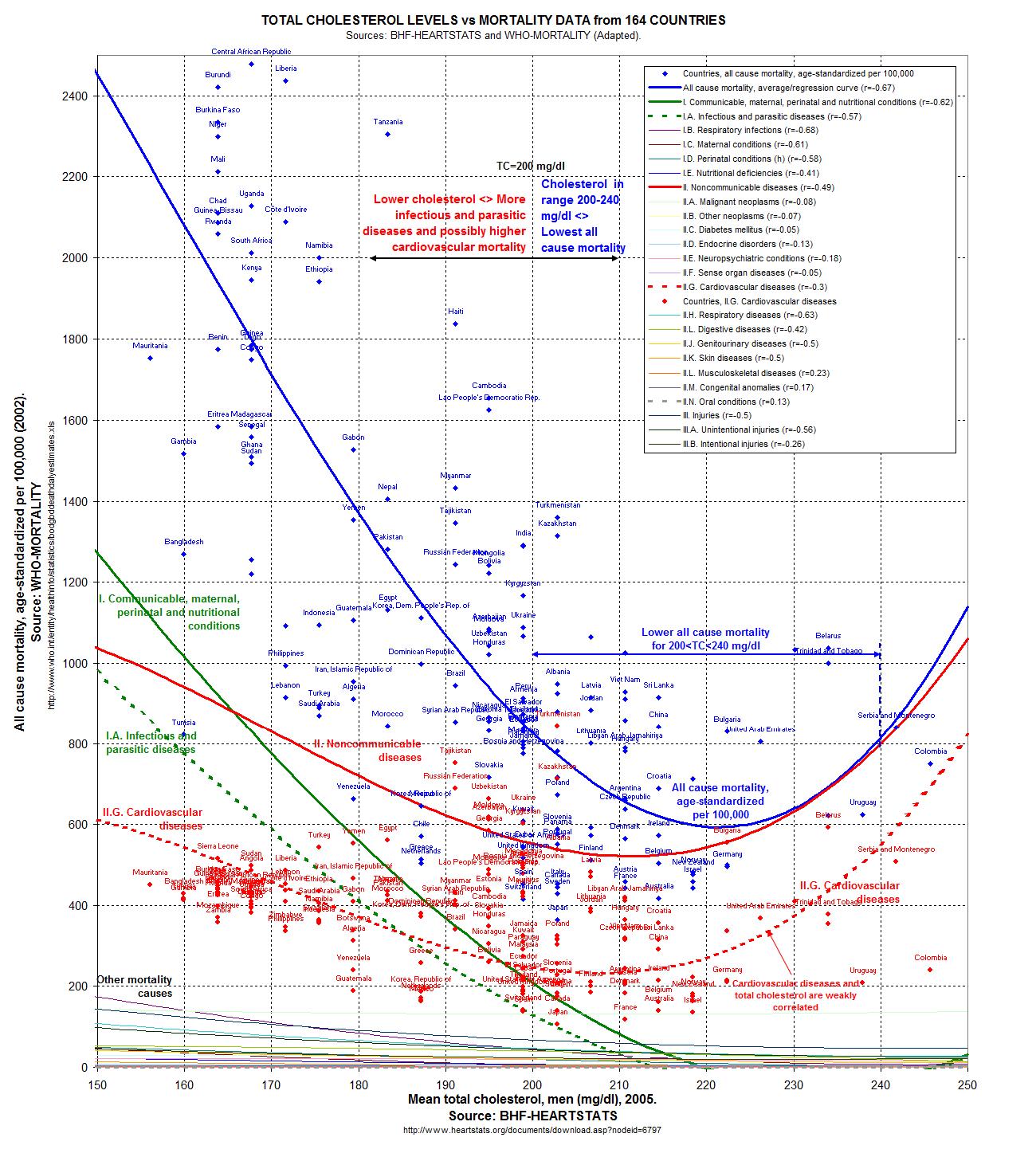
Standard view: Get that TC below 200, or else you’ll have a heart attack or you’ll have to pay a higher health insurance premium, if the insurers take you on at all.
My take: Mostly meaningless. Even though the epidemiological evidence suggests a TC between 200 and 240 mg/dl is best for all-cause mortality,https://www.ncbi.nlm.nih.gov/pubmed/19903920‘>2
There is an advanced lipid test that’s worth getting: ApoB.
Apolipoprotein B
Every single LDL particle has a single ApoB, making ApoB an effective measurement of LDL particle count. By all accounts I could find, ApoB is reliable and accurate. Every LDL particle has one ApoB, and along with TC:HD ratio, ApoB count is a strong predictor of heart disease risk (again, with the caveat that these studies are on populations leading a decidedly unPrimal and highly inflammatory lifestyle).https://www.sciencedirect.com/science/article/abs/pii/S0306987718304729‘>6
But if you’re eating a healthy diet, your performance is good, your body comp is good (or trending that way), your energy and sleep are rock-solid, you don’t have any familial hypercholesterolemia genes—is it really dangerous to have elevated cholesterol numbers?
I don’t know. But I’m skeptical.
For one, “elevated” cholesterol isn’t necessarily linked to heart disease. Sometimes it’s even linked to lower mortality. For instance, in people older than 60, high LDL is associated with lower all-cause and cardiovascular mortality.http://atvb.ahajournals.org/content/20/6/1536.full‘>8https://www.sciencedirect.com/science/article/abs/pii/0891584993900745‘>10
To name a few. Could “high” LDL particles be closer to benign if they’re more resistant to oxidation? I would imagine so. Does resistance mean immunity to oxidation? Absolutely not. Don’t get cocky.
Substantially “elevated” cholesterol, low HDL or high LDL can be a real problem, but they may also just be a symptom of the larger concern rather than the main issue itself. Cholesterol profile can be impacted by other conditions such as hypothyroidism, untreated diabetes or pre-diabetes, pregnancy (surprise!), lactation, stress, liver conditions, heart disease (symptom, not cause of). Even weight loss or fasting can spike cholesterol numbers (turns out burning all that animal fat off your body can have a momentary effect on blood lipids). Talk to your doctor about what your numbers mean in the grand scheme of your health. And see if you can get a read on other markers, like C-reactive protein (an inflammatory indicator), oxidized LDL, and ApoB (or some other marker of LDL particle number).
High cholesterol shouldn’t be ignored, but it’s not the only thing that matters. You have to look at the whole picture. You have to take a step back (or several steps back) and consider everything—not just numbers on a readout.
If you have any more questions about this topic, drop them down below. Thanks for reading, everyone. Take care.
References
- http://perfecthealthdiet.com/wp/wp-content/uploads/2011/06/O-Primitivo-Cholesterol.jpg
- https://www.ncbi.nlm.nih.gov/pubmed/19903920
- https://www.ncbi.nlm.nih.gov/pubmed/19091534
- https://www.google.com/url?sa=t&rct=j&q=hdl%20tg%20ratio&source=web&cd=4&ved=0CE8QFjAD&url=http%3A%2F%2Fcare.diabetesjournals.org%2Fcontent%2F23%2F11%2F1679.full.pdf&ei=mvPxTrDtMY7XiALm8OW5Dg&usg=AFQjCNE3GzGevscRzugAZXArj9BWCqn9eA&sig2=nhtWZ_ze7r3xudNliKrTYQ
- https://www.ncbi.nlm.nih.gov/pubmed/19903920
- https://www.sciencedirect.com/science/article/abs/pii/S0306987718304729
- https://pubmed.ncbi.nlm.nih.gov/27292972/
- http://atvb.ahajournals.org/content/20/6/1536.full
- https://www.ncbi.nlm.nih.gov/pubmed/16470012
- https://www.sciencedirect.com/science/article/abs/pii/0891584993900745
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4940560/
- https://pubmed.ncbi.nlm.nih.gov/21591986/
- https://pubmed.ncbi.nlm.nih.gov/29190851/
- https://pubmed.ncbi.nlm.nih.gov/10451477/
{kind=link}
The post The Definitive Guide to Cholesterol appeared first on Mark’s Daily Apple.
Powered by WPeMatico
Sorry, the comment form is closed at this time.